Diphtheria
| Diphtheria | |
|---|---|
| Classification and external resources | |
 Diphtheria causes a characteristic swollen neck, sometimes referred to as “bull neck”. |
|
| ICD-10 | A36. |
| ICD-9 | 032 |
| DiseasesDB | 3122 |
| MedlinePlus | 001608 |
| eMedicine | emerg/138 med/459 oph/674 ped/596 |
| MeSH | D004165 |
Diphtheria (Greek διφθέρα (diphthera) "pair of leather scrolls") is an upper respiratory tract illness caused by Corynebacterium diphtheriae, a facultative anaerobic Gram-positive bacterium.[1] [2] It is characterized by sore throat, low fever, and an adherent membrane (a pseudomembrane) on the tonsils, pharynx, and/or nasal cavity.[3] A milder form of diphtheria can be restricted to the skin. Uncommon consequences include myocarditis (about 20% of cases) [4] and peripheral neuropathy (about 10% of cases). [5]
Diphtheria is a contagious disease spread by direct physical contact or breathing the aerosolized secretions of infected individuals. Historically quite common, diphtheria has largely been eradicated in industrialized nations through widespread vaccination. In the United States for example, there were 52 reported cases of diphtheria between 1980 and 2000; between 2000 and 2007 there were only three cases[6] as the DPT (Diphtheria–Pertussis–Tetanus) vaccine is recommended for all school-age children. Boosters of the vaccine are recommended for adults since the benefits of the vaccine decrease with age without constant re-exposure; they are particularly recommended for those traveling to areas where the disease has not been eradicated.
Contents |
Signs and symptoms
The respiratory form has an incubation period of 2–5 days. The onset of disease is usually gradual. Symptoms include fatigue, fever, a mild sore throat and problems swallowing. Children infected have symptoms that include nausea, vomiting, chills, and a high fever, although some do not show symptoms until the infection has progressed further. In 10% of cases, patients experience neck swelling, informally referred to as "bull neck." These cases are associated with a higher risk of death.
In addition to symptoms at the site of infection (sore throat), the patient may experience more generalized symptoms, such as listlessness, pallor, and fast heart rate. These symptoms are caused by the toxin released by the bacterium. Low blood pressure may develop in these patients. Longer-term effects of the diphtheria toxin include cardiomyopathy [7] and peripheral neuropathy (sensory type). [8] The cutaneous form of diphtheria is often a secondary infection of a preexisting skin disease. Signs of cutaneous diphtheria infection develop an average of seven days after the appearance of the primary skin disease.
Mechanism

Diphtheria toxin consists of a single protein or polypeptide. Protein breakdown (Proteolysis) yields two fragments (A and B) which are held together by a disulfide bond. The toxin binds to specific sites in the organism to inhibit translation during protein synthesis. The toxin enters the host cell and is hydrolysed by a trypsin-like protease to produce an toxic fragment. Diphtheria toxin is produced by C. diphtheriae only when it is infected with a bacteriophage. The bacteriophage integrates a gene into the bacteria that causes the toxin to be produced.
Diagnosis
The current definition of diphtheria used by the Centers for Disease Control and Prevention (CDC) is based on both laboratory and clinical criteria.
Laboratory criteria
- Isolation of Corynebacterium diphtheriae from a clinical specimen, or
- Histopathologic diagnosis of diphtheria
Clinical criteria
- Upper respiratory tract illness with sore throat
- Low-grade fever (>103°F is rare)
- An adherent pseudomembrane of the tonsil(s), pharynx, and/or nose.
Case classification
- Probable: a clinically compatible case that is not laboratory-confirmed and is not epidemiologically linked to a laboratory-confirmed case
- Confirmed: a clinically compatible case that is either laboratory-confirmed or epidemiologically linked to a laboratory-confirmed case
Empirical treatment should generally be started in a patient in whom suspicion of diphtheria is high.
Treatment
The disease may remain manageable, but in more severe cases lymph nodes in the neck may swell, and breathing and swallowing will be more difficult. People in this stage should seek immediate medical attention, as obstruction in the throat may require intubation or a tracheotomy. Abnormal cardiac rhythms can occur early in the course of the illness or weeks later, and can lead to heart failure. Diphtheria can also cause paralysis in the eye, neck, throat, or respiratory muscles. Patients with severe cases will be put in a hospital intensive care unit (ICU) and be given a diphtheria anti-toxin. Since antitoxin does not neutralize toxin that is already bound to tissues, delaying its administration is associated with an increase in mortality risk. Therefore, the decision to administer diphtheria antitoxin is based on clinical diagnosis, and should not await laboratory confirmation.[6]
Antibiotics have not been demonstrated to affect healing of local infection in diphtheria patients treated with antitoxin. Antibiotics are used in patients or carriers to eradicate C. diphtheriae and prevent its transmission to others. The CDC recommends[9] either:
- Erythromycin (orally or by injection) for 14 days (40 mg/kg per day with a maximum of 2 g/d), or
- Procaine penicillin G given intramuscularly for 14 days (300,000 U/d for patients weighing <10 kg and 600,000 U/d for those weighing >10 kg). Patients with allergies to penicillin G or erythromycin can use rifampin or clindamycin.
In cases that progress beyond a throat infection, diphtheria toxin spreads through the bloodstream and can lead to potentially life-threatening complications that affect other organs of the body, such as the heart and kidneys. The toxin can cause damage to the heart that affects its ability to pump blood or the kidneys' ability to clear wastes. It can also cause nerve damage, eventually leading to paralysis. 40% to 50% of those left untreated can die.
Epidemiology
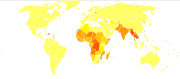
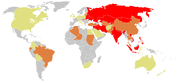
Diphtheria is a serious disease, with fatality rates between 5% and 10%. In children under 5 years and adults over 40 years, the fatality rate may be as much as 20%.[6] Outbreaks, though very rare, still occur worldwide, even in developed nations such as Germany and Canada. After the breakup of the former Soviet Union in the late 1980s, vaccination rates in its constituent countries fell so low that there was an explosion of diphtheria cases. In 1991 there were 2,000 cases of diphtheria in the USSR. By 1998, according to Red Cross estimates, there were as many as 200,000 cases in the Commonwealth of Independent States, with 5,000 deaths.[10] This was so great an increase that diphtheria was cited in the Guinness Book of World Records as "most resurgent disease".
History
In 1878, Queen Victoria's daughter Princess Alice and her family became infected with it, causing two deaths, Princess Marie of Hesse and by Rhine and Princess Alice herself.
In the 1920s there were an estimated 100,000 to 200,000 cases of diphtheria per year in the United States, causing 13,000 to 15,000 deaths per year.[6] Children represented a large majority of these cases and fatalities. One of the most famous outbreaks of diphtheria was in Nome, Alaska; the 1925 serum run to Nome to deliver diphtheria antitoxin is now celebrated by the "Great Race of Mercy".
One of the first effective treatments for diphtheria was discovered in the 1880s by U.S. physician Joseph O'Dwyer (1841–1898). O'Dwyer developed tubes that were inserted into the throat, and prevented victims from suffocating due to the membrane sheath that grows over and obstructs airways. In 1884 Friedrich Loeffler discovered the causative organism (Corynebacterium diphtheriae). In the 1890s, the German physician Emil von Behring developed an antitoxin that did not kill the bacterium, but neutralized the toxic poisons that the bacterium releases into the body. Von Behring discovered that animal blood has antitoxins in it and so he took the blood, removed the clotting agents and injected it into human patients. Von Behring was awarded the first Nobel Prize in Medicine for his role in the discovery, and development of a serum therapy for diphtheria. (Americans William H. Park and Anna Wessels Williams; and Pasteur Institute scientists Emile Roux and Auguste Chaillou also independently developed diphtheria antitoxin in the 1890s.) The first successful vaccine for diphtheria was developed in 1913 by Behring. However, antibiotics against diphtheria were not available until the discovery and development of sulfa drugs.
The Schick test, invented between 1910 and 1911, is a test used to determine whether or not a person is susceptible to diphtheria. It was named after its inventor, Béla Schick (1877–1967), a Hungarian-born American pediatrician. A massive five-year campaign was coordinated by Dr. Schick. As a part of the campaign, 85 million pieces of literature were distributed by the Metropolitan Life Insurance Company with an appeal to parents to "Save your child from diphtheria." A vaccine was developed in the next decade, and deaths began declining in earnest in 1924.[11]
In early May 2010, a case of diphtheria was diagnosed in Port-au-Prince, Haiti after the devastating 2010 Haiti earthquake. The 15 year old male patient died while workers searched for anti-toxin.[12]
References
- ↑ Office of Laboratory Security, Public Health Agency of Canada Corynebacterium diphtheriae Material Safety Data Sheet. January 2000.
- ↑ Corynebacterium diphtheriae only produces diphtheria toxin when lysogenized by beta phage
- ↑ Ryan KJ, Ray CG (editors) (2004). Sherris Medical Microbiology (4th ed.). McGraw Hill. pp. 299–302. ISBN 0838585299.
- ↑ Havaldar, PV; Sankpal MN, Doddannavar RP. (2000). "Diphtheritic myocarditis: clinical and laboratory parameters of prognosis and fatal outcome.". Ann Trop Paediatr. 20 (3): 209–15.. PMID 11064774.
- ↑ Solders, G; Nennesmo I, Persson A. (1989). "Diphtheritic neuropathy, an analysis based on muscle and nerve biopsy and repeated neurophysiological and autonomic function tests.". J Neurol Neurosurg Psychiatry 52 (7): 876–80.. doi:10.1136/jnnp.52.7.876. PMID 2549201.
- ↑ 6.0 6.1 6.2 6.3 Atkinson W, Hamborsky J, McIntyre L, Wolfe S, eds. (2007). Diphtheria. in: Epidemiology and Prevention of Vaccine-Preventable Diseases (The Pink Book) (10 ed.). Washington DC: Public Health Foundation. pp. 59–70. http://www.cdc.gov/vaccines/pubs/pinkbook/downloads/dip.pdf.
- ↑ Havaldar, PV; Sankpal MN, Doddannavar RP. (2000). "Diphtheritic myocarditis: clinical and laboratory parameters of prognosis and fatal outcome.". Ann Trop Paediatr. 20 (3): 209–15.. PMID 11064774.
- ↑ Solders, G; Nennesmo I, Persson A. (1989). "Diphtheritic neuropathy, an analysis based on muscle and nerve biopsy and repeated neurophysiological and autonomic function tests.". J Neurol Neurosurg Psychiatry 52 (7): 876–80.. doi:10.1136/jnnp.52.7.876. PMID 2549201.
- ↑ The first version of this article was adapted from the CDC document "Diphtheria - 1995 Case Definition" at http://www.cdc.gov/epo/dphsi/casedef/diphtheria_current.htm. As a work of an agency of the U.S. Government without any other copyright notice it should be available as a public domain resource.
- ↑ "Diphtheria in the Former Soviet Union: Reemergence of a Pandemic Disease". CDC, Emerging Infectious Diseases. 1998-10-01. http://www.cdc.gov/ncidod/eid/vol4no4/vitek.htm.
- ↑ "United States mortality rate from measles, scarlet fever, typhoid, whooping cough, and diphtheria from 1900–1965". HealthSentinel.com. http://www.healthsentinel.com/graphs.php?id=14&event=graphs_print_list_item. Retrieved 2008-06-30.
- ↑ "CNN's Anderson Cooper talks with Sean Penn and Dr. Sanjay Gupta about the threat of diptheria in Haiti.". CNN.com. http://www.cnn.com/video/#/video/world/2010/05/07/ac.penn.gupta.haiti.med.supply.cnn. Retrieved 2010-05-09.
Further reading
- Holmes RK, "Diphtheria and other corynebacterial infections". In Harrison's Principles of Internal Medicine, 16th Ed. (2005).
- "Antitoxin dars 1735 and 1740." The William and Mary Quarterly, 3rd Ser., Vol 6, No 2. p. 338.
- Shulman ST, "The History of Pediatric Infectious Diseases", Pediatric Research. Vol. 55, No. 1 (2004).
|
|||||||||||||||||||||||||||||||||||||||||